

THE DOCTOR'S BAG
The blog about 19th Century Medicine and Surgery
By Keith Souter aka Clay More
TREPHINATION AND HEAD INJURIES

Last week, knowing my interest in the history of medicine, Jacquie Rogers drew my attention to a post on Facebook about a 5,000 year old cow's skull from an excavation in France. It had a surgically created hole in the right side. No bone healing had taken place, so it was suggested that this was either an early attempt at veterinary surgery, or it was a practice attempt by an ancient surgeon before attempting a trephination on a human, possibly after a head injury.
Head injuries are common in tales about the Old West. That is not surprising, considering all those gunfights, fist-fights and falls from horses. The town doctor on the frontier would probably have to be adept at treating them. That could include trephining the skull - effectively, opening the head.

Treatment of a skull injury from Fieldbook of Medicine 1517
Nowadays we have CT and MRI scans which can give us sophisticated images of the body. A CT scan stands for Computerised Tomography, which involves taking x-rays of the brain from various angles, which are analysed by a computer to build a 3-d image of the brain. This will show any fracture or haemorrhage. A MRI scan stands for Magnetic Resonance Imaging. It uses magnetism, ultrasound and computerised technology to build up images of the inside of the body. These can show the tissues and any abnormalities in surprising detail.
Back in the Old West there were no such luxuries. X-rays were only discovered by William Roentgen in 1895. The first use of them diagnostically only started the year after when Dr John Hall-Edwards in Birmingham, England started to use the technique. The town doctor had to use his clinical skills.
The unconscious patient
The doctor would assess the patient, by examining the scalp for a wound or local bruising. He would examine the ears and nostrils for bleeding, both of which could indicate a significant head injury, with fracture of skull bones.
Coma is the state of absolute unconsciousness when the patient does not respond to any stimulus. Squeezing the ear lobe or using the knuckles of the hand to rub over the sternum (breast bone) are extremely painful and usually will evoke a response in someone who is in a semi-coma. This means that they only respond to painful stimuli. A full coma patient will not even respond to pain.
The pulse would be taken frequently, say every 15 minutes in an unconscious patient. A slowing of the pulse is called bradycardia and may indicate internal hemorrhage somewhere, possibly inside the skull.
The semi-conscious patient
The patient may well be confused, so the level of confuse would be assessed. A rule of thumb gives mild, moderate or severe states of confusion.
Mild - some coherent conversation is possible
Moderate - out of touch generally, but will answer with name or occupation
Severe - no sensible answers given, but will respond to simple commands such as hold my hand.
Deepening confusion may indicate hemorrhage. Sudden vomiting may also be highly significant.
Examination of the cranial nerves
There are twelve paired nerves which come directly out of the brain to supply the head and neck and some of the internal organs. These are separate from most other nerves, which come out from the spinal cord.
1st nerve - olfactory nerve - sense of smell
2nd nerve - optic nerve - vision
3rd, fourth and sixth nerves - occuolomotor, trochlear and abducent nerves move the eye and operate the pupils - get the patient to follow the finger and also shine a light in the eyes - the pupils should constrict
5th nerve - trigeminal nerve - sensory to the face and operates the masseter muscles, the large muscle that moves the jaw - tested by asking to clench the jaw
7th, facial nerve - movements of the face - ester by asking to see the teeth
8th, acoustic nerve - for hearing. Can he hear?
9th glossopharyngeal nerve - to the pharynx - cannot be tested
10th vagus nerve - multiple internal functions, but also moves the palate - tested by asking the patient to say 'Ah.' The palate should move when he does
11th nerve - accessory nerve - tested by asking to shrug the shoulders
12th nerve - hypoglossal nerve - moves the tongue.
Significantly the movements should be equal on both sides. One sided results could indicate a problem with one side of the brain.
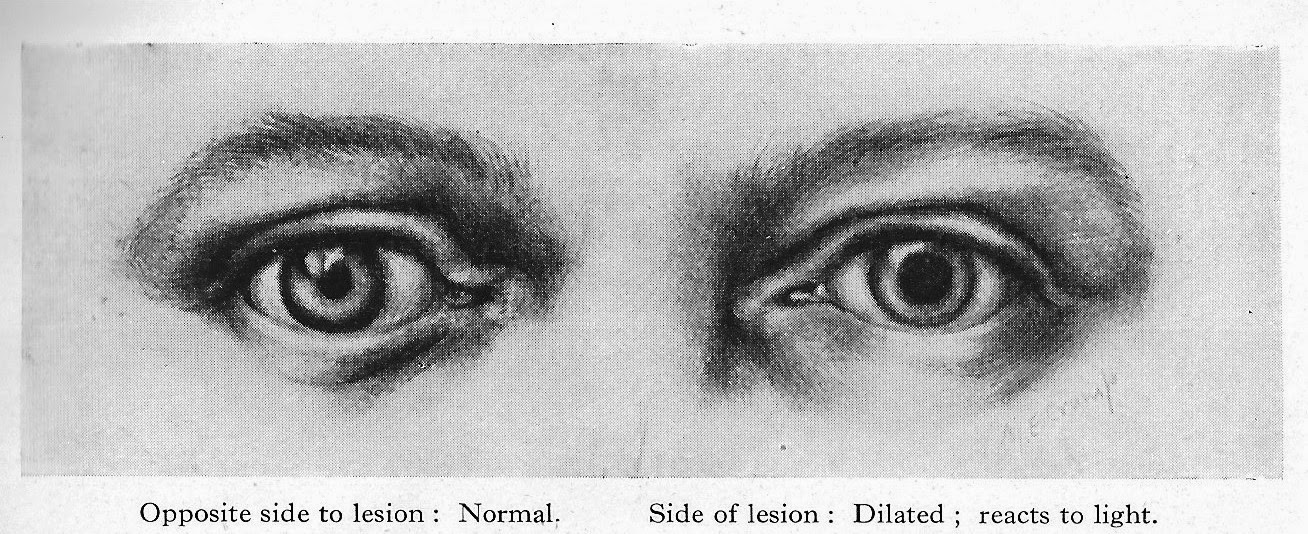
Hutchinson's pupils
These are a set of guidelines devised by Sir Jonathan Hutchinson (1823-1913), a professor of Surgery at the Royal College of Surgeons of London. He wrote a ten volume Archives of Surgery between 1885 and 1899.

Hutchinson's pupil, described by him indicates that an intracranial mass (a tumour or blood clot) will result in a fixed (meaning it will not change size even when light is shone on the eye) and dilated pupil on the same side. This is very significant, since it would indicate where to make the trephination.
Racoon eyes and Battle's sign
Basal skull fractures, that is, fractures of the bones that make up the base of the skull, including the temporal bone, occipital bone, ethmoid and sphenoid bones, can be associated with particular bruising.

Racoon eyes
Battle's sign, named after the English surgeon William Henry Battle (1855-1936) is bruising that occur can behind the ear, again some hours after a basal fracture. Like the racoon eyes it is not necessarily a sign of trauma where it appears, but a sign of a basal skull fracture.

Battle's sign
Your frontier doctor might not have known of them by those names, but he may well have known from past experience, or war service, that they could be of significance.
General physical examination
Here the focus is on assessing the power of each limb and comparing one see of the body with the other. Disparity between the sides could indicate developing or developed paralysis.
Also testing the reflexes with a 'patella or tendon hammer.' The following reflexes are tested:
Biceps tendon by tapping the tendon in the hollow of the elbow.
Triceps tendon by tapping the tendon on the back of the elbow when the elbow is flexed.
Patella tendon by tapping underneath the stella (kneecap) with the leg flexed.
Achilles tendon by tapping the tendon at the back of the ankle.
Lack of reflexes on one side would be significant.
Trephination
The words trephination and trepanation are used interchangeably, since both come from the Greek trypanon, meaning 'to bore.' Archaeological evidence shows that trephination, the boring of a hole in the skull was used in early tribal societies. It was presumably thought that this would let out evil spirits. Examination of many skulls which have been trepanned in this way shows that healing of bone around the site of the boring took place, indicating that in many cases the operation was a success. Incredibly, they used three methods - cutting, scraping and drilling.
The oldest trepanned skull was found at a neolithic burial site at Ensisheim in France. It has been dated to 7,000 years ago.
The reason that it could have helped is by releasing the pressure upon the brain, which would follow a hemorrhage. Unfortunately, in those people who were not suffering from a rise in pressure it may have done actual harm.
The ancient Egyptians had actually developed a quite sophisticated system of medicine and surgery with doctors who specialised in one area of the body. thus they had eye doctors, stomach doctors and head surgeons.
The Edwin Smith papyrus, written in about 1500 BC, is essentially an ancient Egyptian textbook of surgery. It describes surgical instruments and techniques and discusses 48 cases of injuries, including head injuries.

The Edwin Smith Papyrus c 1500 BC - an ancient Egyptian textbook of surgery
A beautiful description of ancient Egyptian surgery is given in the 1945 historical novel The Egyptian by the Finnish writer Mika Waltari, which became an international bestseller and later a Hollywood blockbuster in 1954. In the novel the main character Sinuhe, who became royal physician to Pharaoh Akhenaten (father of Tutankhamen), is apprenticed to Ptahor, the 'opener of head.' He shows him how to examine a patient and diagnose where there may have been a problem in the head from an assessment of the state of consciousness and the use of the limbs. He then shows him how to remove a piece of skull and replace it with a silver plate which is bound with bandages while they await recovery.

Ancient Greek surgical instruments. Note the trephine in diagram 'a' with a central pin
The technique of trephination was also used by the Greeks and the Romans. The instruments required became increasingly sophisticated.
We're going to have to open his head
The experience of British surgeons with gunshot winds to the head during the the Crimean War (1853-1856) was not promising. Trephination was associated with an extremely high mortality of over 95 per cent. George H B Macleod, the chief surgeon of the British Expeditionary Force advise against the operation.
During the American Civil War the operation was performed with better results. The survival rate improved to more than 20 per cent. Then after Lister's aseptic techniques were accepted, recovery rates continued to improve.
In 1882 Samuel W Gross wrote a textbook A System of Surgery, in which he quoted a 41 per cent recovery rate after gunshot trephination.
The trephination operation
The instruments needed:
Trephine - a cutting instrument with a cylindrical blade - usually with a cutting circle of one inch

An antique trephine with horn handle
Chisel and mallet

Rongeur - a strong forceps for grasping bone

Also needed would be a scalpel and various forceps for holding tissues, a gouge for smoothing roughed or fractured bone edges and an elevator to lift the bone disc that was cut.
The operation
The patient's head would be shaved and washed. After Lister this would have been with carbolic soap and then it would be scrubbed and washed with a 1 in 20 solution of carbolic acid in alcohol.
The head would be supported on a sandbag and sterilised towels applied around the site to open the skull. In the earlier frontier days, this would not have been thought necessary.
When a wound already exists and a fractured spicule was apparent, the cite would be exposed by enlarging the wound. When the scalp was not wounded, as in a clubbing head injury or from a fall, then a semilunar flap of skin would be cut and raised. It would be cut so that the free end would point downwards. It would be a shallow curve, carefully made to avoid the main scalp arteries.
Alternatively, a V-shaped incision could be made, again with the V pointing downwards. It should be so arranged as to allow free-draining of blood.
The incision should be carried down to the bone and the tissues helped with forceps. Then the flap would be turned upwards. A suture would be placed through it so that the flap could be held out of the operative territory.
Any bleeding vessels would be secured with pressure forceps to close the vessels off.
Any spicules of fractured bone could be chiseled off with the chisel and mallet.
If there is no fracture, then the circular trephine is applied. The central pin could be bored into the bone, then the trephine is made to cut into the skull by light, sharp movements from left to right and from right to left.
At first bone dust is dry, but it soon becomes soft and bloody. Once through the bone, the pressure changes dramatically.
The area must be kept free of bone dust by irrigation with saline.
The trephine is then gently rocked back and forth to allow it to move, then the elevator is inserted. The ronguer forceps can then be applied carefully to remove the disc.
The blood or the blood clot can then be removed. It may well express itself. The area needs to be irrigated and any bone spicules or bone dust removed.
The bone disc is placed in a china cup and soaked with warm (sterilised) water, ready to be replaced.
Once replaced the skin flap is brought back into place with silkworm-gut sutures.
In later years a spiral rubber tube could be used to drain between the sutures.
It wasn't always a head injury
Abscesses could also cause raised intracranial pressure and need trephination.

Choosing the site of trephination was important, since you need to avoid the middle meningeal artery. The diagram shows the areas that were commonly used. They would avoid the area between A and B, since the artery runs underneath the cranium. Points A and B would be used if a middle meningeal artery haemorrhage was suspected.
This sort of hemorrhage can cause an epidural haematoma. This is a blood clot forming between the dura mater (the thick outer layer of the meninges, the membranes that cover the brain) and the cranium. Rupture of the middle meningeal artery is often the cause. It comes on after a head injury when someone is knocked unconscious. They then recover, seem to regain lucidity and even go off and resume normal activities. Later on they very quickly go drowsy and lose into unconsciousness s the clot forms. It is a life-threatening event and the trephination could be life-saving.
Finally, a case!
Report of a Case of Fracture of the Skull treated by trephining - by Ira Perry, Assistant Surgeon, US Army
Jesus Soldaeo, a Mexican, while at a drunken revel in Brownsville, Texas, June 1, 1866, was struck wit the stock of a gun, which used extensive contusion and fracture of the skull from the external angle of the orbit of the left eye toward the occiput. the fracture could be traced through the scalp distance of six inches........The patient as admitted to the post hospital totally unconscious, with slow pulse and very feeble. The case being considered hopeless, water dressings only were applied....on the third day, the patient being still alive, the trephine was applied, and fragments of bone elevated; three days later the patient was slightly conscious....Until the tenth day the patient had taken nothing but cold water, and now was given some gruel; bowels were opened for the first time.....On June 25th consciousness returned completely and a gradual improvement took place. July 17th the wound was almost healed, and the patient was removed fro the hospital by his friends.
Be bold!
I have used trephination in some of my western stories. It is tough surgery performed in life and death situations, so the operator has to be bold. Which of course, all of us as western writers have to be.
***

Keith, you know how much I love this book. It's fascinating stuff, and I am so glad you put all this information together in this book--it's just perfect for those of us who write, complete with pictures and diagrams and wonderful explanations in layman's terms as well as all the proper medical jargon we need to know to be accurate. Your posts are always fascinating, and this book is one that I use a LOT!
ReplyDeleteThanks, Cheryl. Practising medicine in those days would really have demanded that doctors honed their diagnostic skills. No x-rays, scans or blood tests. Nowadays we rely more and more on high tech investigations, so that even the stethoscope can be replaced by a smart phone.
DeleteWhat a wonderful article, detailed and well-researched. I am familiar with Trepination and to see it explained in this context is fascinating.
ReplyDeleteOh, and I just bought your book.
DeleteThank you for your kind words. I always hope that people will find these articles of some use.
DeleteAnd thank you for buying the book!
DeleteKeith,
ReplyDeleteI have this book, and I refer to it often. It is an invaluable reference in my writing. I’ve also gifted this book to an aspiring western romance writer. I look forward to your monthly articles. Thank you for sharing from your well of knowledge.
Thank you, Kaye. That’s good to know it has helped. And thank you for gifting it. I hope your recipient finds it useful.
DeleteGreat post, Keith.
ReplyDeleteYou are indeed,a multi talented man.
Your presentation of complicated medical terms and procedures are very understandable to we laymen.
Thank you.
You are a gentleman, Jerry. One of the things I live about the Westetn Fictioneers is the range of interests among the members. The WF blog is a great asset, because you can always find a post about something you want to research.
DeleteAbsolutely every western writer should buy your book! I refer to it often (convenient because it's both digital and print). Thanks so much for being so helpful. And a great guy, too.
ReplyDeleteA most interesting and in-depth article. I feel that I've reached at least a novice brain surgeon level. I just need to sharpen my chisel. Thanks for posting Keith.
ReplyDeleteYou are welcome, Gordo. I’ll send your medical degree by air mail! That chisel could save a life one day.
DeleteHa ha. I wondered if you would see it, Jacquie! You are way too kind - and also a great gal ( can one say that?)
ReplyDeleteSo informative, as usual. Although not the same, the husband of one of the women doctors I've been researching lived after a fall in the mine in the Cripple Creek/Victor area aound 1900. The newspapers say he was scalped from the lengthly fall. The family tells me, that although he survived, he wasn't quite right after that.
ReplyDeleteI'll have to mark this post for further info and of course consult your book, which is just to my left here at the computer. Doris
Thanks, Doris. Gosh, what a horrid injury. In fact, I’m planning an article on scalping.
DeleteAlways learn so much from you; mainly that I don't much of anything about doctoring! Please look up Josiah Wilbarger, Bastrop, TX, for your scalping article if you have time.
DeleteThanks, Vicky. I was aware of Joseph Wilbarger and will be referring to him. It really was a. Awful thing to happen.
DeleteAnother very useful article Keith - I also refer to your book quite often while writing. It's on my "Often Used" research shelf!
ReplyDeleteThanks, JES. That’s so good to hear.
DeleteI am so happy to hear about your book, Keith and read this excellent article. I am ordering this book today and will be relieved to finally have an excellent reference book for my writing.I look forward to catching up on more of your articles.
ReplyDeleteThank you, Elizabeth. I truly hope you find it useful in your stories. Thank you for getting it.
DeletePlease Guide me about it. Is is helpful to cure dent in skull. I'll be very thankful to you.
ReplyDelete